

The Injury That Resets the Scale
The Edge Protocol - How to manage severe injury without losing physical capacity, psychological stability, or momentum.

Double hernia. Broken leg. ACL. Multiple knee, ankle, hamstring and groin injuries. 87 stitches across my face. A glass bottle to the back of the head. Hobbling Sunday to Wednesday on a bad achilles tendon for years after every game.
A history like that builds a reference library for pain. Real pain. Not conceptual pain. And then comes the injury that resets the scale. The one where your entire catalog of prior suffering becomes context, not comparison.
The back injury is that one for me right now.
Back pain at a severe level behaves differently from other injuries. A torn ACL is localized, almost honest about where the problem is. Stitches are mechanical. Back pain radiates. Then it colonizes. Because the spine sits at the center of how the body functions, shifting position becomes a negotiation between what you want to do and what the injury will permit.
The worst pain of your life also tends to arrive at the worst psychological moment. You’re not just managing pain. You’re confronting limits you didn’t know existed.
And for anyone who has spent years building their life around physical competence, that confrontation goes deeper than the injury itself.
The Part Nobody Names
Serious injury threatens identity because competence is usually physical before it’s psychological. You realize, lying there, how much of your confidence was quietly built on the assumption that your body would cooperate. That it would show up. That it would perform.
When it stops, recovery becomes partially physical and partially existential. You’re not just rebuilding tissue. You’re rebuilding the version of yourself that assumed physical competence was permanent.
That’s the part most recovery content skips entirely. It’s also the part that determines whether people actually come back or whether they quietly adjust downward and call it acceptance.
Heat and Cold
Most people reach for ice or heat on instinct without understanding what they’re doing physiologically. The sequencing matters more than the choice. Cold belongs in the acute phase, controlling inflammation and numbing tissue, while heat belongs in the subacute and chronic stages where the goal shifts to circulation and repair. [1]
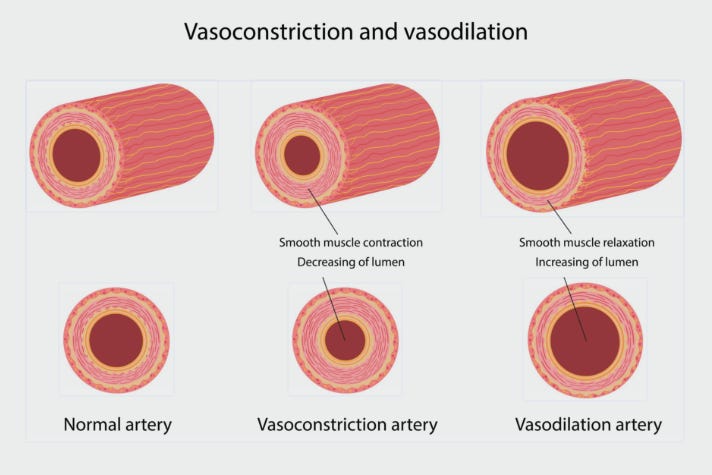
One thing worth knowing: heat applied too early doesn’t just feel wrong, it makes the injury worse. Heat causes vasodilation. It opens blood flow to the area. In acutely inflamed tissue that’s not recovery, it’s acceleration in the wrong direction. Cold for the first 48 hours. Heat after the acute window closes.
Cold therapy can shorten muscle recovery time by 25 to 40 percent in sports medicine applications, while heat improves long-term flexibility by reducing muscle adhesion. [2] They target different phases of the same problem. Use them accordingly.
The Edge
There is no safe, comfortable path back from serious injury. There are two failure modes and a narrow band of correct behavior between them.
Too much too fast: reinjury, re-inflammation, regression. Too passive: atrophy and fear calcify into a new baseline that sits permanently below where you were.
With my ACL I was two weeks late into therapy. By the time I started, scar tissue had already formed and they had to break it up manually. As unpleasant as it sounds. But full commitment once it started produced a surgically repaired right knee that ended up stronger than the untouched left one. The knee that went through surgery, missed time and brutal scar tissue work outperformed the original.
That’s what lives on the other side of the edge.
The goal isn’t rest until it’s gone.
The goal is load until it starts to heal.
Protect and reduce load in the acute phase. Once that window closes, reintroduce movement progressively. Distinguishing between pain that’s protecting and pain that’s signaling damage is the whole game.
Medication
Post-trauma pain management has consistently underweighted individualized risk assessment and non-pharmacological strategies alongside medication. [3] Most people assume medication handles the pain and everything else is optional. Wrong frame.
Medication buys you a window. What you do in that window determines how the recovery goes.
Physical dependence on opioids can develop within days of consistent use, and abrupt discontinuation after even a short period can trigger significant withdrawal and psychological distress. [4] Use it with precision. Enough to function, not enough to feel comfortable. Plan the taper with your doctor before you’re already in the position of needing one.
Medication that removes pain is not the same thing as medication that supports recovery.
The Psychology
The research on mindset during recovery is specific enough to be worth understanding rather than dismissing.
Psychologically resilient individuals experience lower pain catastrophizing day to day, independent of actual pain intensity, because positive emotion interrupts the cognitive loops of rumination and helplessness that sustained severe pain produces. [5]
Pain catastrophizing is what happens when the brain projects the current pain state forward indefinitely. You’re not just hurting today, you’ll hurt forever, something has permanently changed. That loop amplifies the signal. It’s a predictable neurological response to sustained severe pain, not a character flaw.
The people who recover best psychologically aren’t the ones who avoid pain. They’re the ones who stop turning it into an identity.
Get someone involved who understands pain psychologically. Not because the pain is imaginary, but because the mental response to it determines whether recovery is full or partial. [6]
What It Actually Looks Like
A jagged graph that trends upward if you manage it correctly. Some days feel like regression and aren’t. Some sessions hurt more than rest would have because you’re actually working.
Manage the acute phase with precision. Track it, communicate with the right people, don’t wait and hope. Once the acute window closes, load it. Push to the appropriate edge and hold there.
Cold, then heat, in the right sequence. Medication as a tool with a plan attached. Therapy committed to fully, not selectively. A mindset kept constructive because the evidence says it changes outcomes, not because it feels natural.
Pain isn’t the test. Reconstruction is.
The Edge Protocol: Field Summary
0 to 48 Hours Cold. Reduce inflammation. Protect the tissue. No heat.
After the Acute Phase Restore movement carefully. Introduce heat. Begin loading again.
Medication Use enough to function. Never enough to disappear.
Mindset Pain is information, not prophecy.
The Edge Avoid both extremes: recklessness and passivity. Find the narrow band between them. Return to it daily.
This article is part of Performance Protocol, a system for building a body and mind that holds when life doesn’t. performanceprotocol.ai
Sources
[1] Results Physiotherapy. Heat and Cold Therapy in Injury Prevention and Pain Management. 2025. https://www.resultspt.com/blog/posts/heat-and-cold-therapy-in-injury-prevention-and-pain-management
[2] Cao et al. Clinical Applications and Potential Mechanism of Cold Acclimation Therapy. PMC, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12285887/
[3] Smith et al. The Effect of a Life Care Specialist on Pain Management and Opioid-Related Outcomes. PMC, 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8626911/
[4] HHS Guide. Patient-Centered Reduction or Discontinuation of Long-term Opioid Analgesics. PMC, 2020. https://pmc.ncbi.nlm.nih.gov/articles/PMC7145754/
[5] Sturgeon & Zautra. Psychological Resilience Predicts Decreases in Pain Catastrophizing Through Positive Emotions. PMC, 2013. https://pmc.ncbi.nlm.nih.gov/articles/PMC3626095/
[6] Chua et al. Reviewing Psychological Practices to Enhance Psychological Resilience in Chronic Pain. Springer, 2025. https://link.springer.com/article/10.1007/s11916-025-01373-4